What is Anterior Shoulder Instability?
Anterior shoulder instability, also known as anterior glenohumeral instability, is a condition in which damage to the soft tissues or bone causes the head of the humerus (upper arm bone) to dislocate or subluxate from the glenoid fossa, compromising the function of the shoulder. It is caused by trauma or injury to the glenohumeral joint in which the upper arm bone is dislodged from its usual position in the middle of the glenoid fossa. Anterior shoulder instability accounts for 95 percent of all acute traumatic shoulder dislocations.
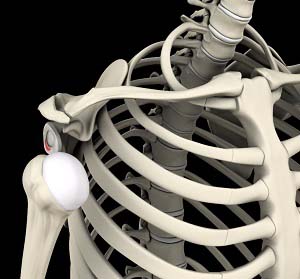
Anatomy of the Shoulder
The shoulder joint (glenohumeral joint) is a ball and socket joint. A ball at the top of the upper arm bone (the humerus) fits neatly into a socket called the glenoid, which is part of the shoulder blade (scapula). The labrum is a ring of fibrous cartilage surrounding the glenoid, which helps in stabilizing the shoulder joint. Tendons and ligaments around the shoulder joint provide additional strength and stability to the joint.
Causes of Anterior Shoulder Instability
Some of the causes and risk factors of anterior shoulder instability include:
- A sudden dislocation injury to the shoulder
- Bankart lesions, an injury of the anterior glenoid labrum
- Humeral avulsion of the glenohumeral ligament (HAGL), an injury to the ligaments that join the upper arm bone to the glenoid
- Rotator cuff muscle weakness
- Hill-Sachs defect, an injury to the cartilage and bone of the humeral head
Signs and Symptoms of Anterior Shoulder Instability
Some of the signs and symptoms of anterior shoulder instability include:
- Persistent glenohumeral joint pain
- A sensation of grinding or popping in the shoulder joint
- Tenderness in the glenohumeral joint
- Swelling and bruising of the shoulder
- Visible deformity and loss of function of the shoulder
Diagnosis of Anterior Shoulder Instability
Anterior shoulder instability is diagnosed with a review of your symptoms, medical history, and a physical examination of the shoulder. Your doctor will assess the extent of injury by palpating the area to check for points of tenderness and checking the range of motion and strength of the shoulder. Imaging studies such as X-rays may be ordered to obtain additional information about the potential causes of the instability and to rule out other causes of shoulder pain. Additionally, a CT scan and/or an MRI may also be ordered for a detailed evaluation of the bones and soft tissues of the shoulder joint.
Treatment for Anterior Shoulder Instability
The treatment options for anterior shoulder instability include both conservative and surgical measures.
Conservative Treatment
- Closed reduction: Following a dislocation, your surgeon can often externally manipulate the shoulder joint, usually under anesthesia, realigning it into proper position.
- Rest: Rest the injured shoulder and avoid activities that require overhead motion. A sling may be worn for 2 weeks to facilitate healing.
- Ice: Ice packs should be applied to the affected area for 20 minutes every hour.
Surgical Treatment
When conservative treatment options fail to relieve shoulder instability, your surgeon may recommend shoulder stabilization surgery. Anterior shoulder stabilization surgery is performed to improve the stability and function of the shoulder joint and prevent recurrent dislocations. It can be performed arthroscopically or through open surgery, depending on your condition.
Arthroscopy is a surgical procedure in which an arthroscope, a small flexible tube with a light and video camera at the end, is inserted into the joint to evaluate and treat the condition. It is a minimally invasive surgery and is performed through 2-3 tiny incisions (portals) made around the joint area. Through one of the incisions, an arthroscope is passed. The camera attached to the arthroscope displays the images of the inside of the joint on the monitor, which allows your surgeon to carry out the required repair accordingly through tiny surgical instruments that are passed through the other incisions.
Open surgery is mostly required to correct severe instability. During this surgery, a large surgical cut is made on the shoulder and the muscles under it are moved apart to obtain access to the joint capsule, labrum, and ligaments. These soft tissue structures are then reattached, tightened, or repaired as needed depending on the extent of tissue injury and closed with sutures.
The surgery is followed by rehabilitation to restore range of motion and strength of the shoulder joint.
Related Topics
- Subacromial Impingement Syndrome
- Rotator Cuff Tear
- Shoulder Pain
- Anterior Shoulder Instability
- Shoulder Impingement
- SLAP Tears
- Arthritis of the Shoulder
- Shoulder Labral Tear
- Shoulder Dislocation
- Little League Shoulder
- Frozen Shoulder
- Shoulder Trauma
- Clavicle Fracture
- Proximal Humerus Fractures
- Sternoclavicular Joint (SC joint)
- Acromioclavicular (AC) Joint Osteoarthritis
- Proximal Biceps Tendinitis
- Internal Impingement of the Shoulder
- AC Joint Separation
- Shoulder Tendonitis
- Partial Rotator Cuff Tear
- Bicep Tendon Rupture
- Shoulder Labral Tear with Instability
- Proximal Biceps Tendon Rupture
- Multidirectional Instability of the Shoulder
- Massive Retracted Rotator Cuff Tear
- Calcification Tendinitis
- Rotator Cuff Pain
